



Contents
Scroll to:
https://doi.org/10.21886/2219-8075-2023-14-3-51-58
Scroll to:
Objective: to study the deep and skin temperatures of the knee joint by microwave radiothermometry (RTM) in healthy girls of comparable age in the pre- and pubertal periods. Materials and methods: the study was carried out in the "Problem Scientific Laboratory of Physical Methods of Diagnosis and Treatment" of Rostov State Medical University and the children's health camp "Mir" (Krasny Desant village, Rostov region). It was 45 girls aged 12 years, taking into account gender development, divided into two groups: 1st gr. (n=28) — prepubertal period; 2nd gr. (n =17) — puberty. RTM of the knee joints was performed according to a certain scheme using the MWR2020 system (ex RTM-01-RES) (Moscow, Great Britain). Results: in the groups, the color fields of deep and skin temperature, when compared, are characterized by a slight geometric and color transformation are similar to each other; the lowest temperature is noted in the projection of the patella. Temperature fields of thermoasymmetry make it possible to reveal temperature differences in groups of subjects. In the 2-nd group, there are also higher growth and weight indicators, lower deep and skin temperature in almost all areas of the knee joint, fluctuations reach 0.4 –1.4 ° C. Conclusion: a decrease in temperature in the knee joints in pubertal girls with a relatively mature menstrual cycle reflects general changes in hormonal regulation in this period of development. When forming the temperature indicators of healthy girls, it is necessary to take into account the hormonal processes of puberty with division into groups of pre- and pubertal periods of development.
Tarakanov A.V., Lebedenko A.A., Ladanova E.S., Tarakanova T.D., Skorodumova E.G., Yatsuk A.N. Microwave radiothermometry of knee joints in girls in pre- and pubertal periods. Medical Herald of the South of Russia. 2023;14(3):51-58. (In Russ.) https://doi.org/10.21886/2219-8075-2023-14-3-51-58
Joint diseases as a multidisciplinary medical problem are especially important and relevant in pediatrics. This is associated with serious disabling diseases, periods of growth in children, increased physical activity, and injuries. Clinically, arthritis is usually accompanied by all the classic signs of inflammation: pain, local hyperthermia, swelling and increase in volume, deformation (defiguration), and impaired movement. Currently, objectivization of the processes occurring in the joints and surrounding tissues in pathology is solved with the help of visualization methods. These are radiologic, ultrasound, and magnetic resonance methods of research. However, they have their positive and negative aspects of application. At the same time, a change in local temperature is one of the earliest signs of almost any inflammation [1][2].
Biological objects are a source of electromagnetic radiation. Its intensity is determined by the rate of metabolic processes, blood circulation, and other factors. Modern medical devices were created that allow specialists to determine the degree of internal radiation; one of them is a passive microwave radiometer. It is used to measure the intensity of internal tissues’ own radiation in microwave and infrared frequency ranges and to register internal temperature and skin temperature indices in different areas of the body under different conditions [3][4][5].
In a review by Laskari et al. (2023), the use of microwave radiothermometry (RTM) was shown to be effective for the differential diagnosis of arthritis and for the assessment of clinical and subclinical inflammation at the individual level of large or small joints and at the patient level. The method showed higher compliance with a musculoskeletal ultrasound investigation, used as a landmark, in comparison with a clinical examination in rheumatoid arthritis [6].
The authors showed a possibility of using the method of microwave RTM in juvenile idiopathic arthritis to assess the dynamics of the disease during treatment on the basis of thermoasymmetry of deep and cutaneous temperatures by temperature fields and fields of temperature differences in the projection of the corresponding morphological structures of the knee joint [7]. It was also suggested to use RTM in complex with generally accepted visualization methods. It would be reasonable to combine imaging methods with RTM as an accessible, simple, non-invasive, and independent method for early detection of the inflammatory process in tissues. RTM allows specialists to determine the development of early inflammation, objectively assess the severity of the inflammatory process in arthritis of various genesis, including juvenile idiopathic arthritis, and timely monitor the effectiveness of therapy [6][8].
The analysis of the previously obtained results of RTM of knee joints in healthy children showed that there were no significant temperature differences in boys and girls aged from 8 to 11 years old. The analysis of the data on deep and skin temperature in girls aged 11–13 years revealed a significant scatter of data [7]. These facts were associated by the authors with hormonal events in the body of girls, which cannot but affect the level of metabolic processes. The appearance of menarche at this age indicates the beginning of the active formation of reproductive function and the transition of the organism to another level of metabolism. Along with changes in the bone structure, height and weight change, and the load on the joints increases, which probably also causes changes in metabolic processes and blood circulation in them. The question of whether bone traction coincides with changes in circulation and increased metabolism remains open. The need to perform the work in the transition age period is also necessary to form a reference group of healthy children for the comparative analysis of temperature data in children with diseased joints.
The aim of the study was to investigate the depth and skin temperature of knee joints by microwave RTM in healthy girls of comparable age in the pre- and pubertal periods of development.
The study was carried out at the “Problem Scientific Laboratory of Physical Methods of Diagnosis and Treatment” of RostSMU and on the basis of children’s health camp “Mir” (Rostov Region, Krasny Desant Village). The protocol of the local independent ethical committee of RostSMU No. 9 is dated September 27, 2018. A total of 45 girls aged 12 years old were examined. Taking into account their age and sexual development according to Tanner, the girls were divided into Group 1 (n = 28, prepubertal period) and Group 2 (n = 17, pubertal period). RTM of skin and depth temperature of knee joints was performed in both groups. In Group 2, the study was conducted between Day 5 and Day 12 of the menstrual cycle. The paper presents temperature data of the left knee joint as the “non-dominant” leg.
RTM was performed using the MWR2020 (ex RTM-01-RES) system (Moscow, UK) with a two-channel antenna. RTM is based on the contact measurement of microwave radiation power of the human body using special antenna applicators. The system is approved for clinical use in the countries of the former Soviet Union and has CE class I marking. It operates in the frequency range from 1 to 4 GHz, the diameter of the antenna applicator is 39 mm, and the declared accuracy is ±0.2 °C for both deep and skin temperature.
The method is safe, non-invasive, and passive, which evaluates the in vivo temperature of internal tissues. The measurement depth is from 3 to 7 cm [3]. The methodology of the measurement: the child is lying on the back; the knee joint area was adapted to the optimal room temperature (23–26 °C) for 5–7 minutes [9].
Nine radio sensors (Figure 1) were placed according to a certain scheme: knee joints from the front, the zone on the right, then, the zone on the left with symmetric temperature estimation. Skin temperature was registered in the same projection as internal temperature, practically simultaneously. The total time of the study of two knee joints was 10–12 minutes. Morphological landmarks included the central zone (zone 5) – patella and lower 3 placements (zones 7–9) – joint projection [7].
Statistical processing of the results. In the beginning, the sampling was tested for the normality of distribution using the Shapiro-Wilk test. If the significance coefficient was p≥0.05, the null hypothesis that the sampling had a normal distribution was accepted. Parametric Student’s t-test was used to compare the values of indices in groups. In the absence of normal distribution, the Mann-Whitney test was used. When comparing the indicators between Group 1 and Group 2, the samples were independent. Differences were considered statistically significant at p ≤ 0.05. The tables show Me – median and [Q1, Q3] – interquartile interval (25% and 75% percentiles).
The analysis of the main somatometric indicators showed that the weight of girls in Group 1 was significantly (p<0.05) lower (41.3±2.3) than in Group 2 (50.0±3.3). A similar tendency was observed for height indices, which were 151.5±3.2 cm in Group 1 and 160.7±4.1 cm in Group 2 (p<0.05). Body mass index in Group 2 (19.3±0.9 kg/m²) was also higher (p<0.05) compared to Group 1 (18.0±0.8 kg/m²). The steps of RTM tests and the analysis of the obtained data were carried out according to a certain algorithm. After the evaluation of deep and skin temperature and their registration by the device, temperature fields and thermoasymmetry fields were analyzed (Figures 1, 2). Further, the numerical parameters were analyzed, and their statistical difference was assessed (Table 1).
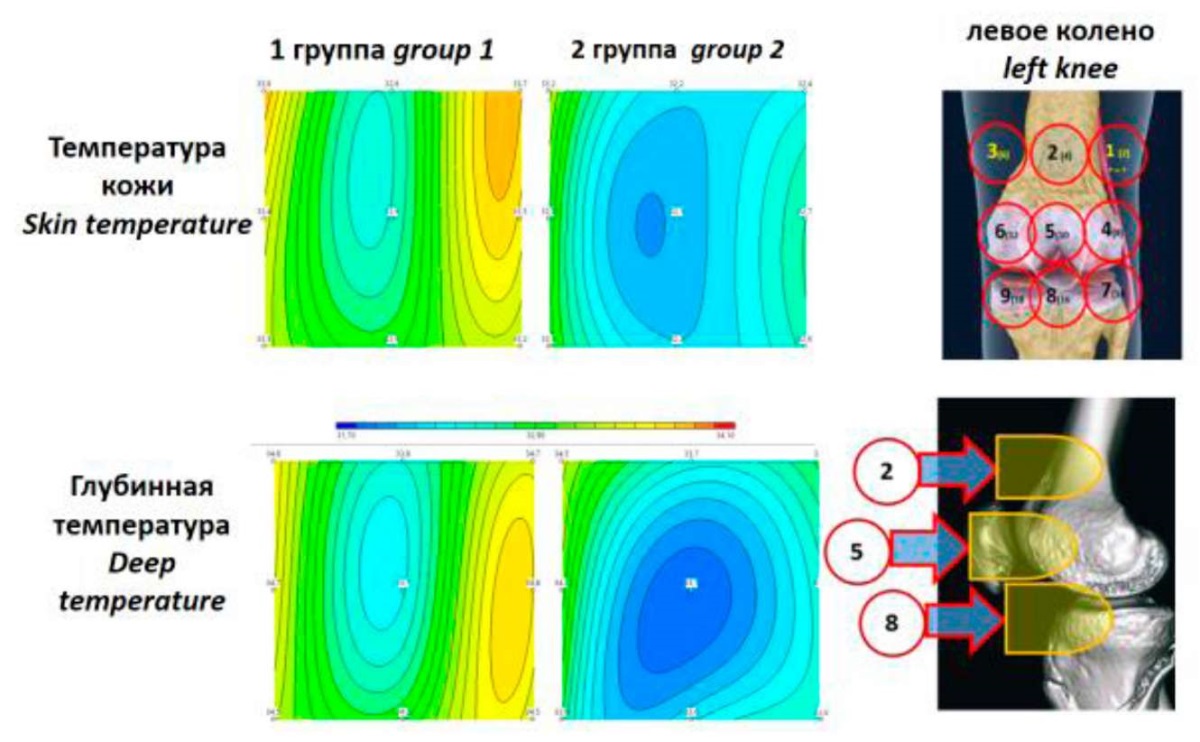
Figure 1. Temperature fields of the skin and deep temperature
of the left knee joint in 12-year-old girls (Groups 1 and 2).
The figure on the right shows the scheme of measurement zones.
The significance of temperature data between groups is shown in Table 1.
During the visual assessment of the temperature fields of the deep temperature of the left knee joint in girls with a relatively well-established menstrual cycle (Group 2) and in the absence of menarche (Group 1), the majority of “cold” places (light blue and blue colors) were recorded above the kneecaps. The same pattern is noted for skin temperature. The majority of “warm” zones (yellow color) are registered in girls without menarche (Group 1) on the outer surface of the thigh (zones 1 and 4 of measurements). Visualization of the deep and skin temperature fields revealed a similar color pattern. The analysis for temperature asymmetry showed that in Group 2 (Figure 2), a lower temperature was noted, and its difference in some zones reached 1.4 °C. This applies to the outer surface of the joint of girls without menarche, where the highest temperature was noted. Group 2 girls had the lowest temperature in the inner surface of the knee joint (zones 6 and 9), the similarity of the color pattern and symmetry were lost.
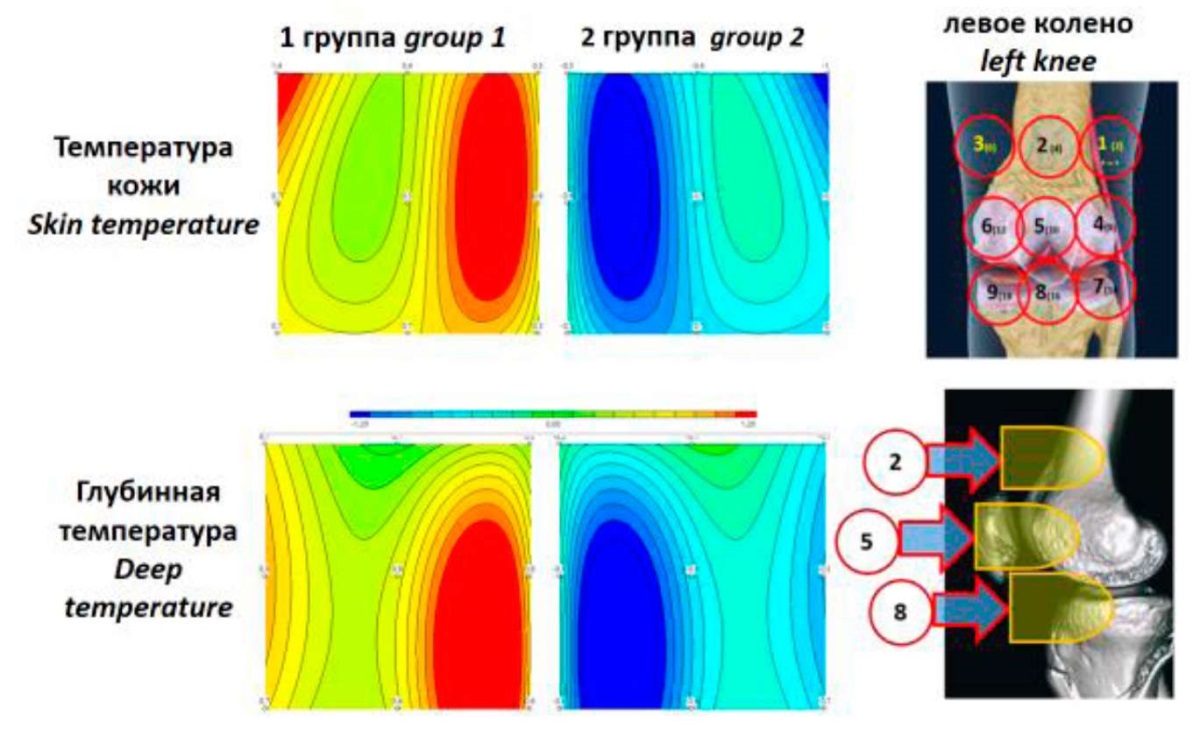
Figure 2. Temperature fields of skin thermoasymmetry and deep temperature
of the left knee joint in 12-year-old girls (Groups 1 and 2).
The figure on the right shows the scheme of measurement zones.
The significance of temperature data between groups is shown in Table 1.
Further, a statistical analysis of the radiothermometric data indices of deep and skin temperatures was carried out. The RTM parameters of skin and deep temperatures in Groups 1 and 2 are presented in Table 1. It follows from the table that practically all the indicated parameters in both groups have a significant statistical difference. At the same time, in the projection of the articular gap – the medial meniscus and articular surface of the medial condyle of the femur (zone L9) and attachment of the cruciate ligaments (zone L8), the depth temperature values were insignificantly lower in Group 2. The internal temperature values were also insignificant in the projection of the femur (zone L2).
Table 1
Skin temperature and deep temperature in the region of the left knee joint
in girls with and without menarche, (°C)
|
Groups |
n |
Age |
Skin temperature measurement zones |
||||||||
|
L1 |
L2 |
L3 |
L4 |
L5 |
L6 |
L7 |
L8 |
L9 |
|||
|
1 – Girls of the prepubertal period |
28 |
12 [ 12;12] |
33.7 [ 33.1;33.9] |
32.6 [ 32.0;32.8] |
33.8 [ 33.2;34.0] |
33.5 [ 33.1;33.7] |
32.6 [ 32.1;32.9] |
33.4 [ 33.0;32.7] |
33.2 [ 32.8;33.6] |
32.9 [ 32.5;33.1] |
33.3 [ 32.8;33.5] |
|
2 – Girls of the pubertal period |
17 |
12 [ 12;13] |
32.4 [ 32.2;33.1]* |
32.2 [ 31.9;32.8]* |
33.2 [ 33.5;33.6]* |
32.7 [ 32.1;34.4]* |
32.1 [ 31.2;32.8]* |
32.9 32.0;33.4]* |
32.6 [ 32.0;33.1]* |
32.2 [ 31.8;33.0]* |
32.7 [ 32.0;32.5] |
|
Deep temperature measurement zones |
|||||||||||
|
1 – Girls of the prepubertal period |
28 |
12 [ 12;12] |
34.7 [ 34.3;35.1] |
33.8 [ 33.6;34.0] |
34.8 [ 34.4;35.0] |
34.8 [ 34.0;35.1] |
33.7 [ 33.4;34.3] |
34.7 [ 34.3;35.0] |
34.5 [ 34.1;34.9] |
34.2 [ 33.6;34.5] |
34.5 [ 32.3;33.5] |
|
2 – Girls of the pubertal period |
17 |
12 [ 12;13] |
34.1 [ 33.7;34.3]* |
33.7 [ 33.6;33,9] |
34.5 [ 34.0;34.7]* |
33.8 [ 33.8;34.9]* |
33.1 [ 32.7;33.8]* |
34.2 [ 33.8;34.6] |
33.8 [ 33.7;34.3]* |
33.6 [ 33.1;34.1] |
33.9 [ 33.5;34.8] |
Note: * – P < 0.05 between Groups 1 and 2.
Because the analysis of the numerical data in Table 1 can be difficult to interpret, the authors presented them as Figure 3 for visualization. Figure 3 shows temperature changes over all measurement zones. Statistical analysis of the indicators revealed that a reliably low depth temperature was noted in the girls of Group 2 in the area of the kneecap (zone 5) and along the outer edge of the joint (zones 1, 4, 7). At the same time, analysis of skin temperature data showed that almost the entire skin above the knee joint in Group 2 girls was significantly colder, except for zone (9) above the medial epicondyle (p>0.05).
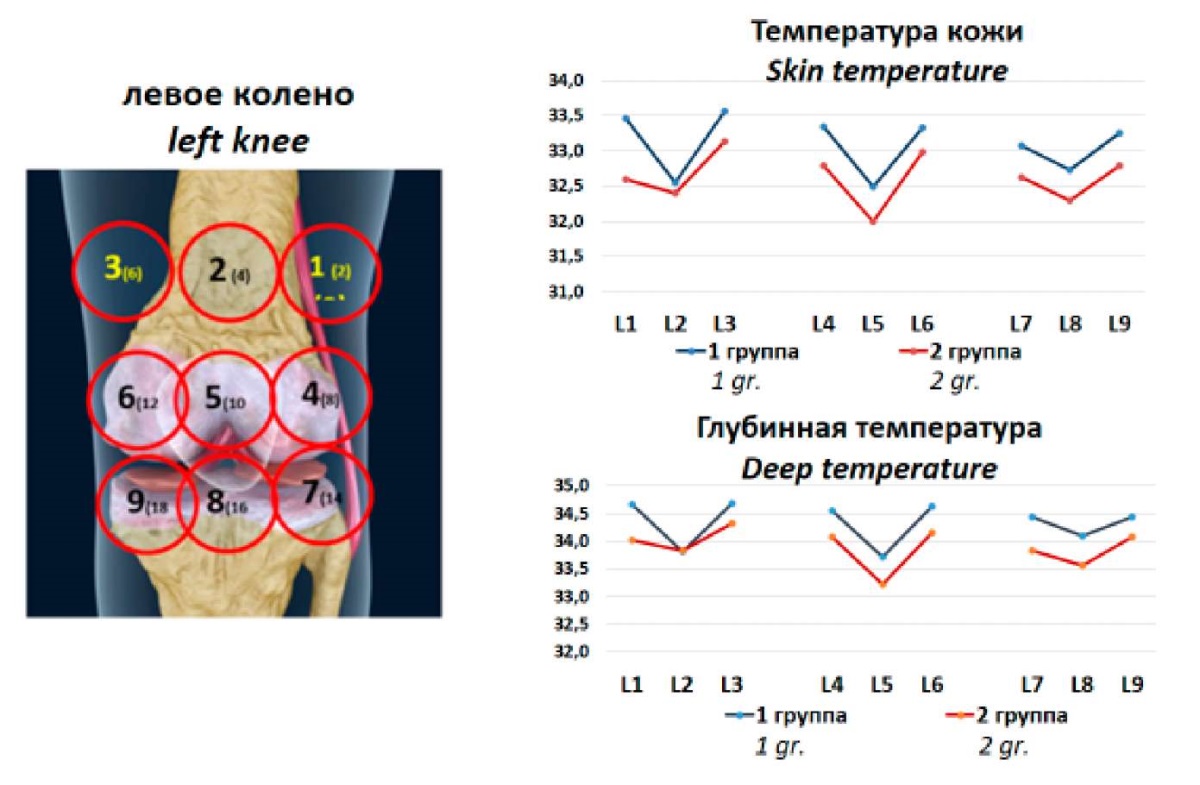
Figure 3. Skin temperature and deep temperature of the left knee joint
in 12-year-old girls – Groups 1 and 2 above the measurement zones.
The figure on the left shows the scheme of measurement zones.
The significance of temperature data between groups is shown in Table 1.
Thus, Figure 3 shows a general pattern of lower temperature in Group 2 girls for both skin and depth temperature.
One of the indicators of children’s health is timely puberty. The physical and hormonal signs of normal puberty are referred to above the age of 8 years in girls (with dark skin at 6–8 years) and 9 years in boys [10]. These figures may vary in different countries. According to Tanner (1997), the average age of onset of puberty in girls in the UK is between 11 and 11.5 years and ranges between 9 years and up to 14.0 years [11].
The key mechanism underlying the transition from pre-puberty to puberty is a decrease in the threshold of hypothalamic sensitivity to the minimum level of estrogens, which was sufficient to inhibit hypothalamic centers, as well as disinhibition of the anterior lobe of the pituitary gland, leading to an increase in gonadotropin (GT) secretion (primarily follicle-stimulating hormone (FSH), and later luteinizing hormone (LH)). The release of GT through a positive “feedback” mechanism leads to the increased production of sex steroids in the gonads, an increase in the number of receptors sensitive to them in the cells not only of the reproductive system organs, but also in many other tissues, including muscle and bone. It also provides a pubertal growth spurt [12].
In the pre-pubertal period, sex and adrenal steroids stimulate the timely growth of mammary glands, skeletal growth, and other physiologically established changes in the girl’s body, typical to this period of development. The completion of a long and consistent functional formation of the hypothalamic-pituitary-ovarian axis is the formation of ovulatory menstrual cycles and maturity of generative function. Estradiol also contributes to the “maturation” of the skeleton, which eventually leads to growth plate fusion and cessation of linear growth. Estradiol levels, from puberty until the onset of ovulatory menstrual cycles, increase from 10 to 156 pg/mL [13]. These hormonal changes during puberty lead to a growth spurt that affects both the axial (trunk) and appendicular (limbs) components. The limbs accelerate before the trunk, with the distal parts of the limbs accelerating before the proximal parts. Thus, the adolescent has “all arms and legs” during early puberty [14].
In the present study, significant changes were found in the main somatometric indices in the groups, especially in body weight and height, which is natural. Compared to adrenarche (physiologic growth spurt), the hormonal regulation of pubertal growth is more complex. In addition to the physiologic influence of factors such as thyroid hormones, cortisol, and insulin, there are important interactions between sex steroids (estrogens and androgens) and the GH (somatotropic hormone)-IGF-1 (insulin-like growth factor) axis that are crucial for normal growth and sexual development.
GH and IGF-I concentrations increase primarily in response to increased estrogen secretion. During the period of the full functioning of the reproductive system, GH secretion and, consequently, circulating IGF-1 concentrations begin to decrease [12]. Later, with the establishment of direct and feedback connections in the hypothalamic-pituitary-gonadal regulatory axis and with their certain physiological sequence of inclusion, menarche comes and hormonal “rearrangements” are no longer so active.
Probably, the decrease in temperature in the knee joints reflects general changes in the hormonal regulation of the reproductive, endocrine, and central nervous systems during puberty. It is also possible that the rapid and intensive growth of the bone system itself outpaces the formation of the blood system of the joints.
When studying the peculiarities of deep and skin temperature indicators of the anterior surface of the knee joint by microwave RTM, to form a reference group of healthy children, it is necessary to take into account the physiological regularities underlying the development and functional changes in the central and peripheral parts of the reproductive system. In the study and comparative analysis of RTM indicators of healthy and sick girls, girls should be divided into groups of pre- and pubertal age, which is justified by the obtained features of RTM indicators depending on the period of puberty with a characteristic for each of them from the functional state of the hypothalamic-pituitary-gonadal system. It was found that girls with the onset of menarche (Group 2) had lower temperatures, both deep and skin, practically in all areas of the knee joint. Higher weight and height indices were observed, which is associated with multiple hormonal and metabolic changes occurring in the body of girls in different periods of puberty.
The emergence of non-invasive and easily accessible methods of assessing internal temperature for diagnosing and monitoring the state of internal organs and joints makes it possible to detect previously undescribed conditions both in norm and pathology. Thus, the performed study showed that when interpreting skin and depth temperatures of knee joints in girls, it is necessary to take into account age, sex, and the period of sexual development.
1. Baranova A.A., Alekseevoj E.I., eds. Revmaticheskiebolezni u detej: klinicheskierekomendaciidlyapediatrov. Moscow: Pediatr`; 2016. (In Russ.)
2. Goryanin I, Karbainov S, Shevelev O, Tarakanov A, Redpath K, et al. Passive microwave radiometry in biomedical studies. Drug Discov Today. 2020;25(4):757-763. https://doi.org/10.1016/j.drudis.2020.01.016
3. Mazepa E.A., Grishina O.V., Levshinskij V.V., Sulejmanova X.M. The unification of microvawe radio thermometry. Mathematical Physics and Computer Simulation. 2017;20(6): 30-50. (In Russ.) https://doi.org/10.15688/mpcm.jvolsu.2017.6.4
4. Shevelev O, Petrova M, Smolensky A, Osmonov B, Toimatov S, et al. Using medical microwave radiometry for brain temperature measurements. Drug Discov Today. 2022;27(3):881-889. https://doi.org/10.1016/j.drudis.2021.11.004
5. Gopalakrishnan K, Adhikari A, Pallipamu N, Singh M, Nusrat T, et al. Applications of Microwaves in Medicine Leveraging Artificial Intelligence: Future Perspectives. Electronics. 2023;12(5):1101. https://doi.org/10.3390/electronics12051101
6. Laskari K, Siores E, Tektonidou MM, Sfikakis PP. Microwave Radiometry for the Diagnosis and Monitoring of Inflammatory Arthritis. Diagnostics (Basel). 2023;13(4):609. https://doi.org/10.3390/diagnostics13040609
7. Tarakanov A.V., Lebedenko A.A., Ladanova E.S., Tarakanova T.D. Prospects for the use of microwave radio thermometry of knee joints in juvenile idiopathic arthritis in children. Sovremenny`eproblemy` nauki i obrazovaniya. 2020;(5);88. (In Russ.) https://doi.org/10.17513/spno.30099
8. Tarakanov AV, Ladanova ES, Lebedenko AA, Tarakanova TD, Vesnin SG, et al. Passive Microwave Radiometry as a Component of Imaging Diagnostics in Juvenile Idiopathic Arthritis. Rheumato. 2022;2(3):55-68. https://doi.org/10.3390/rheumato2030008
9. Tarakanov AV, Tarakanov AA, Vesnin S, Efremov VV, Roberts N, Goryanin I. Influence of Ambient Temperature on Recording of Skin and Deep Tissue Temperature in Region of Lumbar Spine. European Journal of Molecular & Clinical Medicine. 2020;7(1):21-26. https://doi.org/10.5334/ejmcm.274
10. Kaplowitz PB. Precocious Puberty. 2022.
11. Tanner JM, Buckler JM. Revision and update of Tanner-Whitehouse clinical longitudinal charts for height and weight. Eur J Pediatr. 1997;156(3):248-9. PMID: 9083773.
12. Wood CL, Lane LC, Cheetham T. Puberty: Normal physiology (brief overview). Best Pract Res Clin Endocrinol Metab. 2019;33(3):101265. https://doi.org/10.1016/j.beem.2019.03.001
13. Vetvik KG, MacGregor EA. Sex differences in the epidemiology, clinical features, and pathophysiology of migraine. Lancet Neurol. 2017;16(1):76-87. https://doi.org/10.1016/S1474-4422(16)30293-9
14. Kelly A, Shults J, Mostoufi-Moab S, McCormack SE, Stallings VA, et al. Pediatric Bone Mineral Accrual Z-Score Calculation Equations and Their Application in Childhood Disease. J Bone Miner Res. 2019;34(1):195-203. https://doi.org/10.1002/jbmr.3589
Alexander V. Tarakanov - Dr. Sci. (Med.), Professor, Head of department of emergency medicine (with a course of military and extreme medicine), Rostov State Medical University.
Rostov-on-Don
None
Alexander A. Lebedenko - Dr. Sci. (Med.), Professor, Head of the Department of Pediatric Diseases No. 2, Vice-Rector for Pediatrics and Obstetrics, Director of the RostSMU Research Institute, Rostov State Medical University.
Rostov-on-Don
None
Elena S. Ladanova - Assistant of the Department of Propaedeutics of Childhood Diseases Rostov State Medical University.
Rostov-on-Don
None
Tatyana D. Tarakanova - Cand. Sci. (Med.), docent of department of children’s diseases № 2, Rostov state medical University.
Rostov-on-Don
None
Elizaveta G. Skorodumova - Cand. Sci. (Med.), Junior Researcher of the Department of Emergency Cardiology and Rheumatology, Associate Professor of the Training Center of the I.I. Janelidze Research Institute of Emergency Medicine.
St. Petersburg
None
Anastasia N. Yatsuk - 6th year student of the Pediatric Faculty of Rostov State Medical University.
Rostov-on-Don
None
Tarakanov A.V., Lebedenko A.A., Ladanova E.S., Tarakanova T.D., Skorodumova E.G., Yatsuk A.N. Microwave radiothermometry of knee joints in girls in pre- and pubertal periods. Medical Herald of the South of Russia. 2023;14(3):51-58. (In Russ.) https://doi.org/10.21886/2219-8075-2023-14-3-51-58
29, Nakhichevansky Lane, Rostov-on-Don, 344002
Rostov State Medical University
Тel.: +79185710558
e-mail: journal@medicalherald.ru


































