


Contents
Scroll to:
 S. A. Nenadskaya,
E. V. Kovalev,
E. G. Erganova,
N. V. Leonenko,
O. A. Noskova,
V. V. Batashev,
S. Yu. Vodyanitskaya,
I. K. Dorofeeva,
A. S. Chernaya,
A. A. Voloshka
S. A. Nenadskaya,
E. V. Kovalev,
E. G. Erganova,
N. V. Leonenko,
O. A. Noskova,
V. V. Batashev,
S. Yu. Vodyanitskaya,
I. K. Dorofeeva,
A. S. Chernaya,
A. A. Voloshka https://doi.org/10.21886/2219-8075-2024-15-1-44-53
Scroll to:
Objective: to analyze the incidence of healthcare-associated infections (HAIs) in healthcare settings of the Rostov region and the risks of their occurrence in order to develop proposals for improving the complex of anti-epidemic and preventive measures to prevent HAIs in healthcare settings of the Rostov region at present.
Materials and methods: the materials for the work were data from reports "On the state of sanitary and epidemiological welfare of the population in the Rostov region" during 2009–2022, inspection reports and instructions from officials of the Department of Rospotrebnadzor in the Rostov region, expert opinions of specialists from the filial of the Federal Budgetary Healthcare Institution "Center for Hygiene and Epidemiology in the Rostov Region" in Rostov-on-Don on selective inspection of healthcare setting in 2021-2023. The work used an operative and retrospective epidemiological analysis.
Results: the results of the analysis of the incidence of HAIs and the risks of their occurrence in healthcare settings of the Rostov region distinctly demonstrated the relevance of the problem of HAIs. To ensure the safety of medical care in the Rostov region, additional professional training programs about prevention of HAIs have been developed for medical workers.
Conclusion: the results obtained made it possible to identify the risks of HAIs and propose specific measures to improve the complex of anti-epidemic and preventive measures to prevent HAIs in healthcare settings of the Rostov region.
Nenadskaya S.A., Kovalev E.V., Erganova E.G., Leonenko N.V., Noskova O.A., Batashev V.V., Vodyanitskaya S.Yu., Dorofeeva I.K., Chernaya A.S., Voloshka A.A. The risks of healthcare-associated infections in healthcare settings of the Rostov region. Medical Herald of the South of Russia. 2024;15(1):44-53. (In Russ.) https://doi.org/10.21886/2219-8075-2024-15-1-44-53
One of the challenges of modern medical practice is the problem of healthcare-associated infections (HAIs), which cause significant material and social insults, aggravate the condition of patients, increase the duration of their hospitalization, and often lead to disablement and death [1]. In accordance with Sanitary Regulations and Norms (SanPiN) 3.3686-21, “healthcare-associated infections (HAIs) include any infectious disease that has developed in a patient in connection with the delivery of any type of healthcare in a treatment-and-prophylactic institution, as well as cases of exposure of medical employees to infectious diseases resulting from their professional activities”.
Widespread prevalence and negative consequences for the health of patients and medical personnel, as well as for the economic state, rearrange HAIs into a multidisciplinary problem, and its relevance has not diminished for decades [2].
The World Health Organization (WHO) declares that no type of healthcare institution in any country can claim to be free from the risk of HAIs; nevertheless, morbidity can be minimized by managing the risks of their emergence and spread. The risk of developing HAIs is determined by the invasiveness of treatment and diagnostic procedures, the degree of epidemiological safety of medical technologies and the hospital environment, as well as by the features of pathogens and the characteristics of various categories of patients [3].
In Russia, according to official statistics, less than 30 thousand cases of HAIs are registered annually; however, according to experts, the true number may reach 2–2.5 million cases [4]. HAIs can affect up to 5–10% of patients in hospitals over the country. Every patient staying in the hospital for more than 48 hours is at risk of contracting HAIs. The emergence of HAIs increases the duration of hospitalization and treatment costs and also contributes to the formation of a negative attitude of patients toward hospital treatment [5]. The main forms of HAIs are surgical site infections (SSIs), catheter-associated urinary tract infections, catheter-associated bloodstream infections, ventilator-associated pneumonia, infections of newborns, infections of postpartum women, etc. Sources of HAIs are patients, healthcare workers, caregivers, and visitors. Concurrently, cases of HAIs are associated, as a rule, with violations of the requirements of sanitary rules and regulations, sanitary and anti-epidemic regimes, as well as disinfection and sterilization regimes.
The problem of HAIs is inextricably linked with the formation and wide spreading of hospital strains of HAI pathogens, which have multiple resistance to antibiotics and disinfectants; this negatively affects the quality of patient treatment and the efficacy of preventive measures [6]. The most common etiological agents of HAIs are opportunistic microorganisms from the ESCAPE group: Enterococcus, Staph. aureus, Clostridium difficile, Acinetobacter spp., Pseudomonas aeruginosa, and representatives of the Enterobacteriaceae family.
Along with the evolution of medical technologies and prevention methods, the epidemic process of HAIs has also undergone changes [7]. The intensive development and wide spreading of high-tech invasive diagnostic and treatment methods create new risks and determine the demand for the continuous improvement of technologies, methods, and means of prevention, as well as surveillance and verification systems. In order to prevent the emergence and spread of HAIs in medical institutions, sanitary and anti-epidemic (preventive) measures should be carried out, including the implementation of production control, the adoption of isolation measures for patients with HAIs, interruption of transmission routes through disinfection measures, and accomplishment of preventive measures among medical personnel related to preliminary and periodic medical examinations, as well as immunological prophylaxis.
Improving the quality and life expectancy of the population is the main vector of the development of the modern healthcare system. The implementation of this approach is possible through the introduction of new technologies and proper resource support, including financial, material, technical, and technological facilities for medical institutions [8]. In the complex of measures for preventing HAIs in medical institutions, the most important item is the continuous assessment of the state and trends in the development of the epidemic process to determine the reasons for their emergence and timely make executive decisions to ensure adequate measures.
Epidemiological surveillance of HAIs and monitoring of the implementation of mandatory requirements of the legislation of the Russian Federation in the field of ensuring the sanitary and epidemiological well-being of the population and protection of consumer rights are among the main activities of Rospotrebnadzor.
Currently, the activity runs in accordance with the “National Concept for the Prevention of Healthcare-Associated Infections”, approved by the Chief State Sanitary Doctor of the Russian Federation in 2011, as well as the order of the Ministry of Health of the Russian Federation dated November 29, 2021 No. 1108n “On approval of the procedure for carrying out preventive measures, identifying and registering cases of emergence of healthcare-associated infections in a medical institution, the nomenclature of healthcare-associated infections, which are subjected to identification and registration in a medical institution”.
An analysis of the incidence of HAIs in the current period shows that after the peak incidence of HAIs in 2020 associated with the COVID-19 pandemic, when 130,803 cases were registered in the Russian Federation, in the next 2 years, the incidence decreased by 46.76%. In 2022, only 69,645 cases of HAIs were reported. It should be noted that the incidence of HAIs in 2022, excluding cases of COVID-19, increased by 3% compared to the previous indicators; in particular, in 2021, there were 15,373 HAI cases and 15,837 cases in 2022. Furthermore, in the period from 2015 to 2019, the indicator was lower than the long-term average rate (24,655 cases) by 35.8%1.
The morbidity rate among personnel in medical institutions decreased by 35% and amounted to 41,254 cases of HAIs in 2022. Meanwhile, in 2021, the indicator was 63,225 cases; specifically, in the structure of HAIs, the morbidity of medical personnel was 59.2%, and 41,207 cases were caused by COVID-192.
In Russia, the main share of the total incidence of HAIs is registered in surgical and “other” hospitals. It is worth noting that in 2022, the relevancy of surgical hospitals increased; 34.2% of all cases of HAIs were detected in them, while in 2021 this rate was 31.0%. Compared to the “pre-COVID” period, the proportion of HAIs, detected in “other” hospitals, increased; in particular, in 2019, the rate was 26.5% but in 2022 it grew to 44.4%. The share of HAIs registered in inpatient social service institutions as well as in infectious disease hospitals and departments decreased and amounted to 1.9% and 1.6%, respectively, while in 2021, they were 4.0% and 2.1%3, respectively.
In 2022, COVID-19 cases still dominated (77.26%) in the structure of HAIs but their share decreased by 6.91% compared to the previous year, namely in 2021 their share was 84.17%. The second place in the structure of HAIs was held by lower respiratory tract infections (LRTIs) and pneumonia, which amounted to 7.85%; in 2021 they were 5.6%. Before the COVID-19 pandemic, namely in the period between 2015 and 2019, the greatest significance in terms of the average value of their shares had such forms of HAIs as LRTIs (26.8%), SSIs (23.17%), and purulent-septic infections (PSIs) of postpartum women (13.19%) and newborns (10.75%)4.
In 2022, with a decrease in the rate of COVID-19 in the structure of HAIs, the share of other forms increased as follows: the SSI rate was 5.22% versus 2.98% in 2021; the PSI rate in newborns was 2.51% versus 1.88% in 2021; the PSI rate in postpartum women was 2.37% versus 1.71% in 2021; the rate of infections associated with infusions, transfusions, therapeutic injections, and immunizations was 1.38% versus 0.95% in 2021; the airborne infection rate was 1.32% versus 0.75% in 20215.
It is noteworthy that in foreign countries, according to WHO, the share of urinary tract infections is 27–36%, while in the Russian Federation, this rate is 0.84%, which indicates problems in identifying and registering this form of HAIs in the country6.
The purpose of the study is to analyze the incidence of HAIs in the medical institutions of the Rostov Region (RR) and the risks of HAI emergence in order to develop proposals for improving the complex of anti-epidemic and prophylaxis measures to prevent HAIs in the medical institutions of the RR under present-day conditions.
The materials included data from the reports “On the state of sanitary and epidemiological well-being of the population of the Rostov Region” for the period from 2009 to 2022, inspection reports, instructions from officials of the Rospotrebnadzor Office for the Rostov region, and expert opinions of specialists from the branch of the federal budgetary health care institution “Center for Hygiene and Epidemiology in the Rostov Region” in the city of Rostov-on-Don from certain medical institutions of the RR for the 2021–2023 period. The methodological basis of the work was SanPiN 3.3686-21 “Sanitary and epidemiological requirements for the prevention of infectious diseases” and other regulatory documents of the Russian Federation in the field of ensuring the sanitary and epidemiological well-being of the population.
The study used operational and retrospective epidemiological analysis.
In the RR, dynamic tracking of the state of HAIs is constantly carried out within the framework of epidemiological monitoring and state surveillance, and a set of anti-epidemic and preventive measures is arranged and accurately put into practice.
Since 2009, a trend toward an increase in the incidence of HAIs in the Russian Federation has been revealed due to coronavirus infection COVID-19 (Fig. 1). Concurrently, in 2022, the number of HAI cases, excluding COVID-19 cases, decreased by 21.2% compared to 2021 and was 1.7 times lower than the long-term average level over the period from 2009 to 2019.
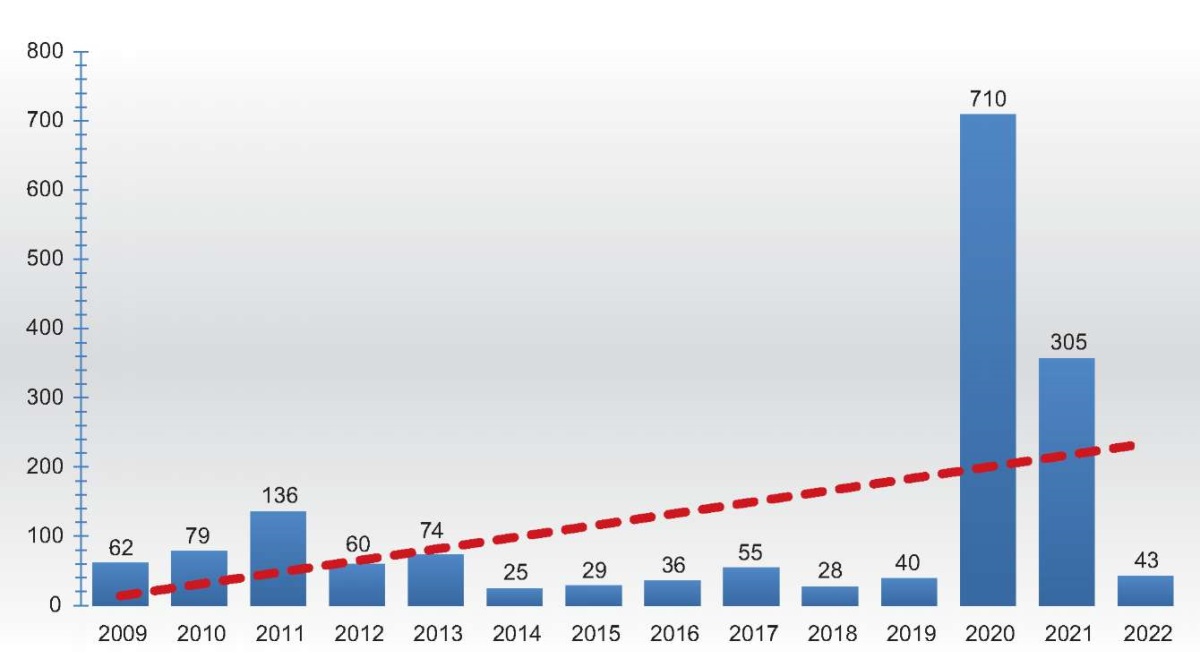
Figure 1. Dynamics of healthcare-associated infections (HAIs) in healthcare settings
of the Rostov region (absolute numbers) for the period 2009–2022.
Рисунок 1. Динамика ИСМП в медицинских организациях Ростовской области
(абсолютные числа) за период 2009–2022 гг.
In 2020, in medical institutions of the RR, the structure of HAIs was dominated by infections caused by SARS-CoV-2 (89.9%) in the form of diseases of the lower respiratory tract, including pneumonia (68.3%), and upper respiratory tract (31.7%) due to the epidemic situation in the region stipulated by COVID-19.
In 2020, similar to the Russian Federation, in the medical institutions of various profiles in the RR, the number of cases of COVID-19 was identified at the maximum level, and their rate was from 50 to 100% of all HAIs. Specifically, COVID-19 was the only HAI, which was registered in surgical and children's institutions, as well as in social service institutions.
The distribution of registered cases of COVID-19 associated with healthcare delivery in 2020 across hospitals and departments of various profiles repeated the ranking of medical institutions according to registered cases in total. The largest number of COVID-19 was registered in “other” hospitals and departments with a rate of 52.7%; in particular, in outpatient clinics, the rate was 24.3%, in surgical hospitals and departments, it was 9.1%, in inpatient social service institutions, it was 8.0%, in obstetric and gynecological institutions, it was 2.0%, in infectious disease hospitals and departments, it was 3.8%, and in children's hospitals and departments, it was 0.2% of cases.
In 2022, in medical institutions of the RR, the share of PSIs of newborns in the structure of HAIs amounted to 30.2%; the rate of PSIs of postpartum women was 25.6%; the rate of SSIs was 13.9%; the rate of infections associated with infusion, transfusion, therapeutic injection, and immunization was 7.0%; other forms of HAIs were represented by COVID-19 and amounted to 23.3% (Fig. 2).
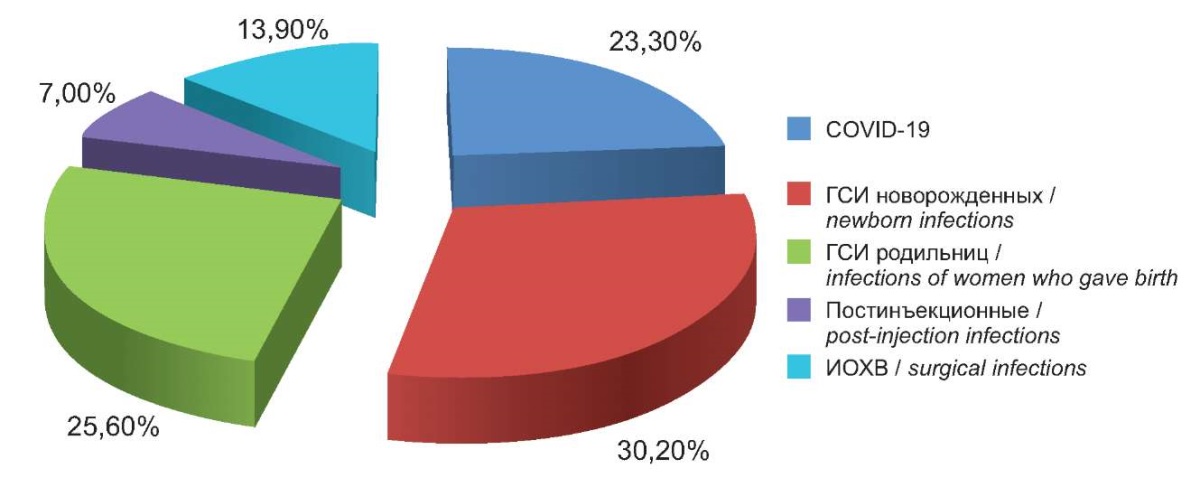
Figure 2. Structure of healthcare-associated infections (HAIs)
in healthcare settings of the Rostov region in 2022.
Рисунок 2. Структура ИСМП в Ростовской области в 2022 г.
The largest share of HAIs in 2022 was registered in obstetrics and gynecology institutions and amounted to 55.8%; in surgical hospitals and departments, the rate was 18.6%; in outpatient clinics, it was 2.3%; in other hospitals and departments, HAI cases were recorded in 23.3% (Fig. 3).
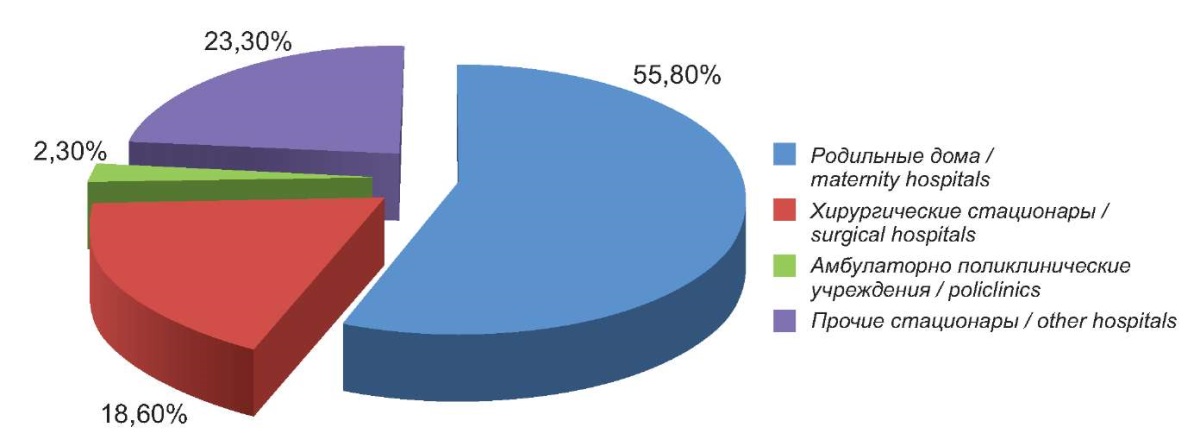
Figure 3. Structure of healthcare-associated infections (HAIs) in Rostov region
according to the profiles of healthcare settings in 2022.
Рисунок 3. Структура ИСМП в Ростовской области
по профилям медицинских организаций в 2022 г.
To determine the risks that stipulate the incidence of HAIs in the RR, inspection reports, instructions from officials of the Rospotrebnadzor Office for the Rostov Region, and expert opinions of specialists from the branch of the federal budgetary healthcare institution “Center for Hygiene and Epidemiology in the Rostov Region” in the city of Rostov-on-Don were examined for the period from 2021 to 2023.
Within the framework of state surveillance in 2022, the results of the conducted laboratory verification on the microbiological examinations of swabs from environmental objects showed that the proportion of non-standard samples in medical institutions generally remained at the level of the previous year and amounted to 0.4%. Concurrently, the situation in obstetric institutions became somewhat more complicated since the number of non-standard samples increased to 1.2% versus 1.0% in 2021. Meanwhile, in children's and surgical hospitals, the situation improved; and non-standard samples were not detected by contrast with data in 2021, when their rates were 1.5% and 0.6%, respectively.
In infectious disease hospitals and departments, outpatient clinics, and dental institutions and departments, non-standard samples were not detected in 2021 and 2022.
In 2022, non-standard samples were not identified upon monitoring the quality of pre-sterilization cleaning of medical devices under state surveillance in maternity hospitals (departments), dental institutions (departments), surgical departments, laboratories, children hospitals (departments), outpatient clinics, infectious disease hospitals (departments), and other institutions.
A bacteriological examination of environmental air as part of state surveillance in 2022 revealed a larger number of non-standard samples, which amounted to 4.2% versus 0.5% in 2021, in certain medical institutions, namely in maternity care institutions and surgical departments.
In 2022, the results of microbiological quality verification in relation to the sterilization of medical products revealed a decrease in the number of non-standard samples by 1.3 times in medical institutions. Nevertheless, non-standard samples were identified in maternity hospitals, surgical departments, and dental and outpatient clinics.
Noteworthy is the deterioration in the quality of disinfectant solutions used in medical institutions and an increase in the proportion of samples unsatisfactory in terms of sanitary and chemical indicators throughout the medical institutions up to 16.3% versus 2.9% in 2021. In particular, in maternity hospitals and departments, this rate was 29.4%, while in 2021, unsatisfactory samples were not identified; in surgical departments, this rate was 14.3% versus 3.0% in 2021, in infectious disease hospitals (departments), it was 25% versus 3.8% in 2021, in dental organizations (departments), it was 7.7% versus 2.7% in 2021, and in outpatient clinics, it was 10.7% versus 3.3% in 2021.
In 2022, no sample inconsistent with requirements was identified in children's hospitals and departments, while in 2021, the rate was 5.8%.
Upon the implementation of surveillance activities during visual inspection, the following typical violations of the requirements of sanitary legislation were identified, including those that were discovered during the development and implementation of production control programs in multidisciplinary institutions:
One should note the importance of the ventilation system in the aerogenic mechanism of transmission of infectious disease pathogens. In this regard, special risks are created due to shortcomings in relation to the disinfection of mechanical inflow exhaust ventilation and air conditioning systems. as well as due to the lack of systematic cleaning and disinfection of filters and heat exchanger chambers of split systems in working rooms.
The submitted documents, namely the acceptance certificate for services, provided by institutions that carried out preventive disinfection of mechanical inflow exhaust ventilation and air conditioning systems, did not reflect the information on the disinfectant used, the rate of its consumption, or the method of its application. That does not allow assessing the safety of performed work. Besides, the disinfection of ventilation and air conditioning systems was carried out by personnel who did not have special training.
In surgical practice, in 69.2% of cases, instruments and dressings serve as factors for the transmission of infectious agents due to the incorrect operation of sterilization equipment, and in 30.8%, of cases due to violations of asepsis by personnel upon working with sterile material [9].
In multidisciplinary medical institutions of the RR, dispensaries, and clinical diagnostic centers, the following situations were revealed:
Flaws in arranging and conducting endoscopic diagnostics were identified:
An important section of the prevention of HAIs is the surveillance of medical institutions of obstetric and gynecological profiles, since infectious diseases pose a significant threat to pregnancy outcomes. In addition to true HAIs, intrauterine infections, acquired intrapartum infections, and infections that developed in women in the postpartum period can emerge in obstetrics and gynecology departments [9]. In the Russian Federation, HAIs registered in maternity institutions are considered one of the significant problems of modern medicine [10].
The following violations of sanitary legislation were identified in obstetric departments of medical institutions in the RR:
Violations of requirements for arranging and conducting disinfection measures in medical institutions were as follows:
During the implementation of planned surveillance activities, as well as upon considering citizen appeals, the following violations of sanitary legislation were identified in the medical institutions of the RR in 2023 in terms of arranging disinfestation, deratization, and acaricidal measures:
During epidemiological investigations of focuses of infectious diseases in medical institutions, the following violations of sanitary legislation were identified:
For the identified violations, officials and legal entities of the medical institutions in the RR were brought to administrative responsibility, and orders of officials of the Rospotrebnadzor Office for the Rostov Region were sent.
The epidemiological analysis of morbidity and the results of verification measures in relation to a number of medical institutions showed the relevance of the problem of HAIs.
The increase in the incidence of HAIs in the RR, as well as over the Russian Federation, is associated with the COVID-19 pandemic. As in the Russian Federation in general, the maximum number of COVID-19 cases was identified in medical institutions of various profiles in the RR in the first year of the pandemic. Meanwhile, the number of HAI cases, excluding cases of COVID-19, in 2022 compared to 2021 decreased by 21.2% and was 1.7 times lower than the long-term average level for the period of 2009–2019.
In 2022, the share of PSIs of newborns in the structure of HAIs amounted to 30.2%; the rate of PSIs in postpartum women was 25.6%; the rate of infections in the area of surgical intervention was 13.9%; the rate of infections associated with infusion, transfusion, therapeutic injection, and immunization was 7.0%; other forms of HAIs were represented by COVID-19 and amounted to 23.3%. By contrast with the Russian Federation, in the RR, PSIs of newborns and postpartum women predominated in the nosological structure of HAIs and amounted to more than half of all HAIs.
Analyzing the distribution of HAI cases by type of medical institutions revealed that the first ranking place in the RR was held by HAIs in obstetric hospitals (departments), which amounted to 55.8% of all registered cases of HAIs; the second one accrued to “other” hospitals with the rate of 23.3%, surgical hospitals were in the third place with the rate of 18.6%. In the Russian Federation, the first ranking place was held by HAIs in “other” hospitals (44.1%); surgical hospitals (34.2%) were in the second place, and obstetric hospitals (12.6%) were in the third place. Moreover, all three categories of medical institutions had high epidemiological significance both in the RR and in the Russian Federation; this share in the RR was 97.7% in total; in the RF it was 90.9%.
There is a connection between the risk of developing HAIs in hospitals of various profiles and the quality of the disinfectants used. There was a sharp increase in the number of non-standard infection samples in terms of sanitary and chemical indicators in maternity (29.4%) and surgical departments (14.3%). An increase in the proportion of detecting unsatisfactory samples of laboratory verification during state surveillance was, presumably, related to the limitation of control and supervision measures.
Upon the development and implementation of production control programs in medical institutions, violations were identified in keeping the effective operation and biological safety of mechanical inflow exhaust ventilation systems; in arranging and recording disinfection and sterilization measures, pre-sterilization cleaning, the flow of their implementation, especially during endoscopic interventions. Besides, sanitary legislation was not kept with regard to the arrangement of disinfestation, deratization and acaricidal measures, etc.
The identified typical violations in the medical institutions of the RR upon visual and laboratory verification made it possible to determine the possible risks of HAIs that formed the basis for the development of proposals for improving the complex of anti-epidemic and preventive measures.
The following priority measures can be recommended for the prevention of HAIs in the medical institutions of the RR:
The results obtained made it possible to identify the main features of HAIs in the medical institutions of the RR with the greatest epidemiological relevancy in obstetric departments, surgical and “other” hospitals, as well as according to nosology attributability. Specifically, in 2020, that was the coronavirus infection COVID-19, and in 2022, that was PSI of newborns and postpartum women. The main risks of HAI emergence were identified, and specific measures were proposed to improve the complex of anti-epidemic and prophylactical measures to prevent HAIs in the medical institutions of the RR.
1. State report “On the state of sanitary and epidemiological well-being of the population in the Russian Federation in 2022”. Moscow: Federal Service for Supervision of Consumer Rights Protection and Human Welfare, 2023. 368 p., p. 246–250.
2. State report “On the state of sanitary and epidemiological well-being of the population in the Russian Federation in 2022”. Moscow: Federal Service for Supervision of Consumer Rights Protection and Human Welfare, 2023. 368 p., p. 246–250.
3. State report “On the state of sanitary and epidemiological well-being of the population in the Russian Federation in 2022”. Moscow: Federal Service for Supervision of Consumer Rights Protection and Human Welfare, 2023. 368 p., p. 246–250.
4. State report “On the state of sanitary and epidemiological well-being of the population in the Russian Federation in 2022”. Moscow: Federal Service for Supervision of Consumer Rights Protection and Human Welfare, 2023. 368 p., p. 246–250.
5. State report “On the state of sanitary and epidemiological well-being of the population in the Russian Federation in 2022”. Moscow: Federal Service for Supervision of Consumer Rights Protection and Human Welfare, 2023. 368 p., p. 246–250.
6. State report “On the state of sanitary and epidemiological well-being of the population in the Russian Federation in 2022”. Moscow: Federal Service for Supervision of Consumer Rights Protection and Human Welfare, 2023. 368 p., p. 246–250.
1. Morozov A.M., Morozova A.D., Belyak M.A., Zamana Yu.A., Zhukov S.V. Infections associated with the provision of medical care. Modern view on the problem (literature review). Journal of new medical technologies, eedition. 2022;(4):107-116. (In Russ.) https://doi.org/10.24412/2075-4094-2022-4-3-3
2. Brusina E.B., Zuyeva L.P., Kovalishena O.V., Stasenko V.L., Feldblium I.V., et al. Healthcare-Associated Infections: Modern Doctrine of Prophylaxis. Part II. Basic Concept. Epidemiology and Vaccinal Prevention. 2018;17(6):4-10. (In Russ.) https://doi.org/10.31631/2073-3046-2018-17-4-10
3. Brusina E.B., Zuyeva L.P., Kovalishena O.V., Stasenko V.L., Feldblium I.V., Briko E.I. Healthcare-Associated Infections: Modern Doctrine of Prophylaxis. Part I. Historical Background. Epidemiology and Vaccinal Prevention. 2018;17(5):17-24. (In Russ.) https://doi.org/10.31631/2073-3046-2018-17-5-17-24
4. Malashenko A.A., Aslanov B.I., Nechaev V.V. Active Epidemiological Surveillance: the Key for Effective Infection Prevention in Pediatric Surgery. Epidemiology and Vaccinal Prevention. 2018;17(6):76–80. (In Russ.) https://doi.org/10.31631/2073-3046-2018-17-6-76-80
5. Krieger E.A., Samodova O.V., Grjibovski A.M. Hospital Surveillance of Healthcare-associated Infections: Repeated Prevalence Surveys. Ekologiya cheloveka [Human Ecology]. 2016;(3):59-64. (In Russ.) https://doi.org/10.33396/1728-0869-2016-3-59-64
6. Naygovzina N.B., Popova A.Yu, Biryukova E.E., Yezhlova E.B., Igonina E.P., et al. Optimization of the system of measures to control and prevent infections associated with the provision of medical care in the Russian Federation. Epidemiology and infectious diseases. Current items. 2018;(1):6-14. (In Russ.) eLIBRARY ID: 32816927
7. Brusina E.B., Kovalishena O.V., Tsigelnik A.M. Healthcare-Associated Infections: Trends and Prevention Prospectives. Epidemiology and Vaccinal Prevention. 2017;16(4):73-80. (In Russ.) https://doi.org/10.31631/2073-3046-2017-16-4-73-80
8. Gelnina T.P., Brusina E.B. Efficiency of Epidemiological Monitoring in Prevention of Helhcare-Associated Infections. Epidemiology and Vaccinal Prevention. 2019;18(3):84-88. (In Russ.) https://doi.org/10.31631/2073-3046-2019-18-3-84-88
9. Priputnevich T.V., Lyubasovskaya L.A., Shuvalova M.P., Baibarina E.N., Sukhikh G.T. Healthcare-associated infections (HAI) in maternity hospitals of Russian Federation (the state of the problem at the beginning of the XXI century). Annals of the Russian academy of medical sciences. 2021;76(2):133-141. https://doi.org/10.15690/vramn1523
10. Zaripova A.Z., Badamshina G.G., Ziatdinov V.B., Isaeva G.S. Epidemiological analysis of neonatal infectious morbidity associated with health care. Kazan medical journal. 2017;98(2):238-243. https://doi.org/10.17750/KMJ2017-238
Svetlana A. Nenadskaya, Senior Lecturer at the Department of Epidemiology
Rostov-on-Don
Evgeny V. Kovalev, Head of the Office; the Chief State Sanitary Doctor in the Rostov Region, Senior Lecturer at the Department of Epidemiology
Rostov-on-Don
Ekaterina G. Erganova, Deputy Head of the Department
Rostov-on-Don
Natalia V. Leonenko, Head of the Epidemiological Surveillance Department
Rostov-on-Don
Olga A. Noskova, Cand. Sci. (Med.), Senior Lecturer at the Department of Epidemiology; Head of the Epidemiology Department
Rostov-on-Don
Viktor V. Batashev, Cand. Sci. (Med.), Associate Professor, Department of Epidemiology
Rostov-on-Don
Svetlana Y. Vodyanitskaya, Cand. Sci. (Med.), Associate Professor, Department of Epidemiology
Rostov-on-Don
Irina K. Dorofeeva, Cand. Sci. (Med.), Associate Professor, Department of Epidemiology
Rostov-on-Don
Anastasia S. Chernaya, Assistant of the Department of Epidemiology
Rostov-on-Don
Artem A. Voloshka, Assistant of the Department of Epidemiology
Rostov-on-Don
Nenadskaya S.A., Kovalev E.V., Erganova E.G., Leonenko N.V., Noskova O.A., Batashev V.V., Vodyanitskaya S.Yu., Dorofeeva I.K., Chernaya A.S., Voloshka A.A. The risks of healthcare-associated infections in healthcare settings of the Rostov region. Medical Herald of the South of Russia. 2024;15(1):44-53. (In Russ.) https://doi.org/10.21886/2219-8075-2024-15-1-44-53
29, Nakhichevansky Lane, Rostov-on-Don, 344002
Rostov State Medical University
Тel.: +79185710558
e-mail: journal@medicalherald.ru


































