



Contents
Scroll to:
https://doi.org/10.21886/2219-8075-2022-13-3-188-192
Scroll to:
Scientifically based and experimentally confirmed data on the morphogenesis of the lymphatic system are necessary to clarify critical periods of development characterized by an increased risk of congenital anomalies of the lymphatic system in order to plan and implement effective prevention, diagnosis and correction of related abnormalities. Among the studied anomalies of lymphatic vessels, lymphangioma is most often mentioned — a congenital benign tumor consisting of many cysts of various sizes. Detection of primary fetal lymphangioma in the early stages of intrauterine development is extremely rare. The purpose of the study: to report a case of early diagnosis of congenital cystic lymphangioma and lymphedema of the left lower limb of the fetus. Congenital (primary) peripheral lymphedema, limb lymphangioma is associated with a malformation of the lymphatic system. Taking into account the fact that operative methods of correction of all types of primary lymphedema are considered unreasonable and ineffective, the main attention requires timely detection of this congenital malformation during screening studies of the fetus and the issuance of recommendations for the management of pregnancy, up to termination for medical reasons. It is necessary to raise the issue of genetic counseling of the couple and conducting the necessary genetic studies. The use of modern diagnostic methods allows for the prevention and treatment of abnormalities in the development of the lymphatic system at an earlier stage of the intrauterine period.
Aksenova O.A., Chaplygina E.V., Kaplunova O.A., Bedarev V.G., Bedarev G.V., Vartanova O.T. Primary lymphangioma, lymphedema of the lower limb of the fetus in the practice of ultrasound. Medical Herald of the South of Russia. 2022;13(3):188-192. (In Russ.) https://doi.org/10.21886/2219-8075-2022-13-3-188-192
Pathology of the lymphatic system in newborns is a little-studied problem in neonatology, which is difficult in the differential diagnosis. The most well-known aspects of this problem are at the intersection of the teachings on immunity, infections, congenital and acquired immunodeficiency states, and pathology of lymphoid organs. However, pathologies of the lymphatic bed, including congenital anomalies of the lymphatic vessels in newborns, are considered a rare deviation, and practitioners are often unfamiliar with the peculiarities of their diagnosis and pathogenesis [1].
The lymphatic system, according to the classical concepts set forth in domestic and foreign educational literature, consists of lymphatic vessels and nodes, being part of the vascular system. It complements the venous system by participating in additional fluid drainage [2].
From the point of view of ontogenesis, at present, due to modern genetic and immunological techniques, as well as the ability to conduct live studies on biological models in vivo, a mixed model of the origin of the lymphatic system has finally been established (from endothelial cells of the cardinal vein and other mesenchymal angioblasts with a distinctive set of markers, from as yet unidentified sources). This indicates a much greater complexity of embryogenesis of the lymphatic system than previously thought [3-5].
Among the studied anomalies of lymphatic vessels, lymphangioma is the most often mentioned one — it is a congenital benign tumor consisting of many cysts of various sizes, which is much less common than hemangioma and accounts for no more than 10–12% of all the benign neoplasms in children, most often located in the neck (95%) [6]. According to other data (Anderson and Kennedy, 1991), 75% of lymphangiomas are located in the neck, 20% — in the axillary region, 2% — in the abdominal cavity and retroperitoneally, 2% affect limbs and bones, and 1% — in the mediastinum [7].
According to Losanoff and Wani, the frequency of this pathology ranges from 1 in 20 thousand to 1 in 250 thousand admissions to a surgical hospital [8][9]. Usually, lymphangioma occurs at the end of the first and (or) the beginning of the second trimester of pregnancy. In 62% of cases, it is associated with chromosomal abnormalities of the fetus and newborn, more often with Turner syndrome. The origin of this tumor has not been fully clarified. It is believed that an etiological factor may be a trauma or an anomaly in the development of the lymphatic system [10].
Lymphedema is a chronic disease of the lymphatic system, leading to a persistent and progressive increase in the size of the affected organ due to the accumulation of fluid with a high protein content in the interstitial space, mainly in subcutaneous fat, due to impaired lymph transport through lymphatic vessels [11]. According to the etiological classification [12], lymphedema can be primary and secondary. The cause of primary lymphedema is congenital abnormalities of the structure of the lymphatic system, such as aplasia, hypo- or vascular hyperplasia. In 80% of cases, the cause of primary lymphedema is the obliteration of distal lymphatic vessels, in 10% of cases — occlusion of the proximal lymphatic vessels of the abdominal cavity and pelvis, and in 10%, there is a failure of the valves of lymphatic vessels. More often, with primary lymphedema, one limb is affected. When both limbs are affected, asymmetry is noted. It occurs more often in girls (70–80% of cases) [12]. There is an opinion [3] that such a pattern of localization of primary lymphedema is explained by the partial origin of the lymphatic system from bipotent angioblasts of the mesenchyma: facts have been found indicating a decrease in the involvement of non-venous sources of development in the embryogenesis of the lymphatic system in the caudal parts of the fetus compared with the cranial parts. This is a possible explanation for the fact that in the initial period, primary lymphedema almost exclusively affects the lower extremities [3][5].
Primary lymphedema may manifest itself both at birth (congenital primary lymphedema) and at any age, but most often during puberty. It is known that it is at least ineffective to treat primary lymphedema with surgical methods, and methods of excision of soft tissues (lipodermatofasciectomy) are considered self-mutilation [11]. Molecular mechanisms of development of the lymphatic system are links in the pathogenesis of many diseases from the group of primary lymphedema, and the influence on these links with the help of gene therapy is currently considered the most appropriate approach [3]. In such conditions, timely detection of congenital lymphopathology with the use of non-invasive or minimally invasive research methods is of particular importance. Ultrasound techniques belong to the methods of the first diagnostic line; it is a simple, accessible method that makes it possible to determine the extent and size of the lesion, assess its structure and localization, determine the presence or absence of blood flow in the affected area, making it possible to differentiate lymphatic malformation from blood vessel malformation [10][13][14].
Screening ultrasound examination in the Russian Federation in accordance with the order of the Ministry of Health of the Russian Federation dated November 1, 2012 No. 572n is carried out three times: at pregnancy terms of 11–14 weeks, 18–21 weeks, and 30–34 weeks1.
The main goal of routine ultrasound examination in the middle of the second trimester of pregnancy is to provide accurate diagnostic information for optimal pregnancy management and the best outcome for the mother and fetus. Another goal is to detect congenital malformations and multiple pregnancies [13].
Although most congenital malformations are detected by ultrasound, it should be borne in mind that some anomalies can be missed even when using the latest equipment by specialists of a high professional level. In addition, some defects may manifest later in pregnancy [14].
The effectiveness of using the method of echography in the diagnosis of congenital anomalies is 70–80%. This visualization method allows detecting anatomical changes in the fetus and making a diagnosis based on the identified picture. However, a certain group of congenital anomalies is not accompanied by gross anatomical abnormalities, or these changes are not so pronounced, and they are not given due attention during routine ultrasound examination (stigma of dysembriogenesis) [13].
The authors of this study analyzed the following clinical case.
Patient M., 37 years old, went to the clinic with a pregnancy period of 20–21 weeks for a screening ultrasound examination. This pregnancy was the fifth one, previous pregnancies ended with urgent childbirth without peculiarities. Obstetric, somatic, epidemiological, and allergological anamnesis was not burdened.
The study was conducted on a high-end SonoAce R7 device (Samsung Medison) with a 2–8 MHz convexic sensor. The fetometric parameters of the fetus corresponded to the period of pregnancy. The sex of the fetus was male.
During the examination, the fetus revealed swelling of the left lower limb. A cystic formation was detected. The thickness of the lower leg area of the left lower limb was 2.3 cm with multiple cystic inclusions; the thickness of the thigh area of the left lower limb was 2.3 cm with cystic inclusions. Pronounced edema of the fetal left foot was detected; the thickness of the foot was 1.8 cm, also with cystic inclusions (Figure 1). The thickness of the right lower limb was not changed, the lower leg was 1.4 cm, the thigh was 2 cm, and the foot was 1.1 cm (Figure 2a, b). Multiple cystic inclusions were detected in the pelvis on the left. The patient was referred for consultation to the Kulakov National Medical Research Center of Obstetrics, Gynecology and Perinatology of the Ministry of Health of the Russian Federation, where the following medical conclusion was issued: the fetus was in a transverse position, its dimensions corresponded to the 21st week of pregnancy, the fetus had cystic lymphangioma of the left lower limb with the involvement of the pelvis, thigh, shin, and foot. The ultrasound picture was pathognomonic for cavernous lymphangioma. It was recommended to conduct a medical consultation and consultation with a perinatal surgeon.

Figure 1. Sonogram of a fetus with lymphedema of the left lower limb, bottom view.
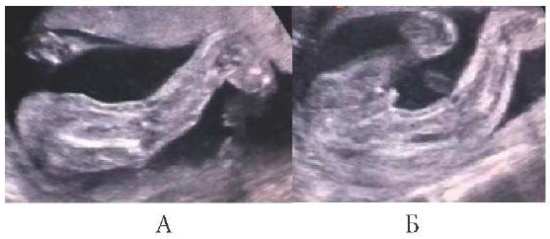
Figure 2. Sonogram of a fetus with lymphedema of the left lower limb, left view
(A — left lower limb with lymphedema; B — the left lower limb with lymphedema and the right unmodified limb of the fetus).
In order to clarify the diagnosis, an intrauterine MR tomography of the fetal body was performed, and the medical conclusion was as follows: pregnancy (week 21), MR picture of retroperitoneal fluid formation on the right side (lymphangioma?) with possible involvement of the gluteal region and the right lower limb (should be differentiated with lymphostasis and fetal edema). A consultation with a pediatric surgeon was recommended.
After all the consultations, a medical consultation was appointed, which was conducted by the specialists of the Federal State Budgetary Institution “Kulakov National Medical Research Center of Obstetrics, Gynecology and Perinatology of the Ministry of Health of the Russian Federation”. A repeated ultrasound of the fetus was previously performed with the following conclusion: progressive pregnancy (20–21 weeks), congenital malformation of the fetus, a liquid multi-chamber formation with dimensions of 34/20 mm visualized in the retroperitoneal space on the right side, blood flow was not registered (lymphangioma), swelling of the soft tissues of the left lower limb. According to the results of the medical consultation, the diagnosis was made “Congenital malformation of the fetus, cystic lymphangioma, lymphedema of the left lower limb (involving the pelvis, hip, shin, foot). Proteus syndrome”.
According to the results of the medical consultation, taking into account the extremely unfavorable prognosis for the life and development of the fetus, as well as the severity and prevalence of the tumor process, termination of pregnancy was recommended.
The diagnosis of “cavernous lymphangioma” was confirmed by a pathoanatomic examination.
The mechanisms of the formation of normal structure variants and the occurrence of human lymphatic system anomalies are still under study. Various conclusions based on the results of such studies are often controversial and contradictory; the reason for this is the complex combinatorial embryogenesis of lymphatic vessels and lymphoid organs. Scientifically based and experimentally confirmed data on the morphogenesis of the lymphatic system are necessary to clarify critical periods of development characterized by an increased risk of congenital anomalies of the lymphatic system in order to plan and implement effective prevention, diagnosis and correction of related abnormalities.
Congenital (primary) peripheral lymphedema, lymphangioma of the extremities is associated with a malformation of the lymphatic system. Taking into account the fact that operative methods of correction of all the types of primary lymphedema are considered unreasonable and ineffective, the main attention requires timely detection of this congenital malformation during screening studies of the fetus and the issuance of recommendations for the management of pregnancy, up to termination for medical reasons. It is necessary to raise the issue of genetic counseling of the couple and conducting the necessary genetic research.
1. Skvortsova V.I. Order of the Ministry of Health of the Russian Federation No. 572n dated November 1, 2012 “On approval of the Procedure for providing medical care in the profile “Obstetrics and gynecology (except for the use of assisted reproductive technologies)”.
1. Mumladze E.B., Eremeeva A.V., Litvak M.M. Trudnosti diagnostiki otjochnogo sindroma u detej rannego vozrasta. Trudnyj pacient. 2007;5(2):17-18. (In Russ.)
2. Shvedavchenko A.I., Oganesyan M.V. Some aspects of the anatomy of the lymphatic system. Journal of Anatomy and Histopathology. 2015;4(3):137-138. (In Russ.) DOI: 10.18499/2225-7357-2015-4-3-137-138
3. Dudnikov A.V., Baitinger V.F., Kurochkina O.S. The development of the lymphatic system in the natural-historical aspect. Part 2. Issues of reconstructive and plastic surgery. 2019;22(2):79-88. (In Russ.). DOI: 10.17223/1814147/69/10
4. Petrenko E. Initial stages of lymphatic system development in ontogenesis. The investigations history in Russia. Bulletin of Science and Practice. 2018;4(2):73–109. (In Russ.) DOI 10.5281/zenodo.1173124
5. Hen G, Nicenboim J, Mayseless O, Asaf L, Shin M, et al. Venous-derived angioblasts generate organ-specific vessels during zebrafish embryonic development. Development. 2015;142(24):4266-78. DOI: 10.1242/dev.129247.
6. Oksenchuk T.V., Belkova T.N., Krivtsova L.A., Katashova E.N., Hrapov D.V., et al. Case of congenital lymphedema in neonatal practice. Pediatria n.a. G.N. Speransky. 2015; 94 (1):149-152 (In Russ.)
7. Anderson NG, Kennedy JC. Prognosis in fetal cystic hygroma. Aust N Z J Obstet Gynaecol. 1992;32(1):36-9. DOI: 10.1111/j.1479-828x.1992.tb01895.x.
8. Losanoff JE, Kjossev KT. Mesenteric cystic lymphangioma: unusual cause of intra-abdominal catastrophe in an adult. Int J Clin Pract. 2005;59(8):986-7. DOI: 10.1111/j.1368-5031.2005.00554.x.
9. Wani I. Mesenteric lymphangioma in adult: a case series with a review of the literature. Dig Dis Sci. 2009;54(12):2758-62. DOI: 10.1007/s10620-008-0674-3.
10. Korbut I.A., Zakharenkova T.N., Nakamura T., Hiroma T. Lymphangioma in the practice of an obstetrician-gynecologist. Problems of health and ecology. Moscow, 2016:108-112. (In Russ.)
11. Makarova V.S. Primary and secondary congenital lymphedema in children. Bulletin of Lymphology. 2014;(4):29-37. (In Russ.) eLIBRARY ID: 25029438
12. Zakharova I.N., Makarova V.S., Tvorogova T.M., Mumladze E.B., Andryukhina E.N. Lymphedemas in pediatric practice. Clinical practice in pediatrics. 2010;5(6):37-42. (In Russ.). eLIBRARY ID: 15575832
13. Plotsky A. R., Drabovich T. V. Mistakes and difficulties in diagnosing malformations during ultrasound. Journal of Grodno State Medical University. 2005;3(11):230-232. (In Russ.). eLIBRARY ID: 19091778
14. Shamshirsaz AA, Stewart KA, Erfani H, Nassr AA, Sundgren NC, et al. Cervical lymphatic malformations: Prenatal characteristics and ex utero intrapartum treatment. Prenat Diagn. 2019;39(4):287-292. DOI: 10.1002/pd.5428
Olga A. Aksenova - Candidate of Medical Sciences, Associate Professor of the Department of Normal Anatomy, Rostov State Medical University.
Rostov-on-Don.
None
Elena V. Chaplygina - Doctor of Medical Sciences, Professor, Head of the Department of Normal Anatomy, Rostov State Medical University.
Rostov-on-Don.
None
Olga A. Kaplunova - Doctor of Medical Sciences, Professor of the Department of Normal Anatomy, Rostov State Medical University.
Rostov-on-Don.
None
Vasily G. Bedarev - student of the pediatric faculty, Rostov State Medical University.
Rostov-on-Don.
None
Grigory V. Bedarev - chief physician of the MC “Rozhdenie”.
Volgodonsk, Rostov Region.
None
Olga T. Vartanova - Candidate of Medical Sciences, Associate Professor of the Department of Normal Anatomy, Rostov State Medical University.
Rostov-on-Don.
None
Aksenova O.A., Chaplygina E.V., Kaplunova O.A., Bedarev V.G., Bedarev G.V., Vartanova O.T. Primary lymphangioma, lymphedema of the lower limb of the fetus in the practice of ultrasound. Medical Herald of the South of Russia. 2022;13(3):188-192. (In Russ.) https://doi.org/10.21886/2219-8075-2022-13-3-188-192
29, Nakhichevansky Lane, Rostov-on-Don, 344002
Rostov State Medical University
Тel.: +79185710558
e-mail: journal@medicalherald.ru


































