


Contents
Scroll to:
https://doi.org/10.21886/2219-8075-2022-13-2-44-49
Scroll to:
Objective: to assess the significance of clinical and anamnestic characteristics of women as risk factors for the development of symphysiopathy during pregnancy.
Materials and methods: a retrospective analysis of 26 birth histories of patients with a diagnosis of symphysiopathy/symphysitis delivered in the GUZ «Clinical Maternity Hospital No. 2» in Volgograd at 38–39 weeks of pregnancy from 2016 to 2020. All patients diagnosed symphysiopathy was made at the management of pregnancy in the antenatal clinic on the basis of complaints, the data of physical examination and by ultrasound. The data of all pregnant women were ordered, encoded and entered into tables in the program MS Excel. Statistical analysis was performed with the SPSS program for windows 16.0.
Results: clinically, symphysiopathy was manifested by pain in the area of the pubic in 100% of cases. According to the medical cards, only two cases (7.7%) were treated with physical therapy. The conducted statistical analysis showed that such risk factors for the development of symphysiopathy as age, parity and body mass index (BMI) do not have statistical significance as possible factors affecting the course of symphysiopathy. A statistical analysis of the possible effect of weight gain on the width of the diastasis was carried out, according to which the compared groups have a statistical difference in the width of the diastasis (p=0.007).
Conclusion: the study shows that there is no significance of such clinical and anamnestic factors as age, parity, BMI for the manifestation of symphysiopathy during pregnancy. In this study, the only statistically significant criterion affecting the course of symphysiopathy is increased overall weight gain during pregnancy.
Vorobyev A.А., Selikhova M.S., Yаkovenko M.S. Symphysiopathy during pregnancy, assessment of risk factors. Medical Herald of the South of Russia. 2022;13(2):44-49. (In Russ.) https://doi.org/10.21886/2219-8075-2022-13-2-44-49
Symphysiopathy is a symptom complex involving pain and diastasis of the pubic bones in the second half of pregnancy. This term replaced the term "symphysitis," emphasizing the inflammatory genesis of the disease, which proved to be incorrect. Data on the prevalence of symphysiopathy are extremely inconsistent, ranging from 0.03 to 2.8% [1][2]. Such contradictions are due to the lack of unified terminology and clear criteria for diagnosis. According to current studies, biomechanical causes, undifferentiated connective tissue dysplasia, and low magnesium and calcium levels underlie the development of symphysiopathy in pregnant women, which in turn, determines the clinical and anamnestic portrait of the woman.
The aim of the study was to assess the significance of women’s clinical and anamnestic characteristics as risk factors for the development of symphysiopathy in pregnancy.
The authors retrospectively analyzed 26 labor histories of patients delivered at the Volgograd Clinical Maternity Hospital No. 2 and 32 labor histories of patients delivered at the Volgograd Regional Clinical Perinatal Center (VRCPC) No. 2 with the diagnosis of symphysiopathy/symphysitis at 38–39 weeks of pregnancy from 2016 to 2020 inclusive. All patients were diagnosed with symphysiopathy during pregnancy management in an antenatal clinic on the basis of complaints, physical examination data, and ultrasound findings.
Data from all pregnant women were arranged, coded, and entered into MS Excel tables. Data with a non-normal distribution were analyzed using the nonparametric Mann-Whitney U-criterion to assess differences between two independent samples. Statistical analysis was performed using SPSS for Windows 16.0.
Because of the lack of unified terminology and generally accepted classification, the criteria for diagnosis differ in different obstetric institutions. Thus, according to the analysis of case histories at Volgograd Clinical Maternity Hospital No. 2, the criteria for the diagnosis of symphysitis/symphysiopathy are pain in the pubic region on palpation, pubic articulation diastasis over 5 mm, symphysis cartilage swelling according to ultrasound. In VRCPC No. 2, the diagnosis criteria are as follows: pain in the pubic area on palpation, diastasis of the pubic joint over 10 mm, swelling of the cartilage of the symphysis according to ultrasound examination.
Clinically, symphysiopathy manifested as pain in the pubic region in 100% of cases. According to the case histories, only two cases (7.7%) attempted treatment with physical therapy. There were no data specifying the type of procedure, as well as the effectiveness of its results. Bandages were recommended in 7 cases (26.9%), the effectiveness of which was also not evaluated. All the women had operative delivery.
When analyzing the birth histories of women with symphysiopathy, the mean age was 27.2±4.6 (19–36) years old. In the age group over 26 years old (n=20, 76.9%), it was diagnosed more frequently than in the 19–25 years group (n=6, 23.1%).
In order to study the possible influence of age on the development of symphysiopathy, the patients were divided into the groups of 19–25 and 26 and more years old according to the age stages of pubic symphysis cartilage mineralization [3][4]. There was no statistically significant difference between the two compared groups in terms of diagnosis time (p=0.632) and diastasis width (p=0.597) (Mann-Whitney U-test for independent samples). The results are shown in the charts (Figure 1).
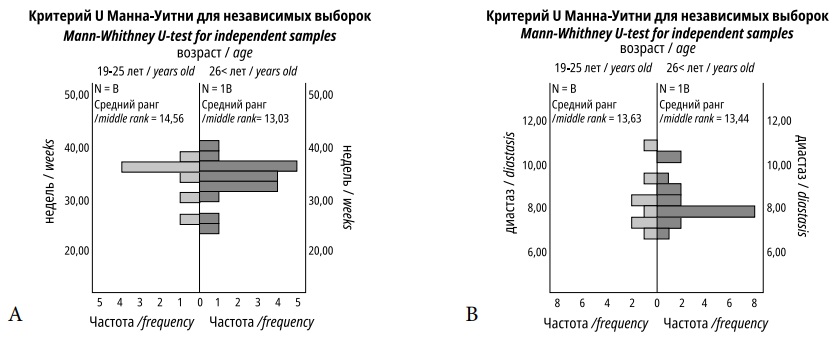
Figure 1. Diagrams showing the distribution of indicators of the period of diagnosis (A), the width of diastasis (B) among pregnant women of 1st group (19–25 years) and 2nd group (26 and more years).
The diagnosis was made at an average of 33.3±3.8 (24–40) weeks of gestation among all pregnant women diagnosed with symphysiopathy.
In order to assess parity as a risk factor influencing the width of the pubic joint diastasis and gestational age at diagnosis, all pregnant women with symphysiopathy were divided into first-born and second-born. The proportion of first-born women was 42.3%. A statistical analysis was performed, which revealed no significant differences between the study groups in the timing of diagnosis (p=0.716) and diastasis width (p=0.619), as clearly illustrated in the charts (Figure 2). It should be noted that in those women who were diagnosed with symphysiopathy in a previous pregnancy, the time of diagnosing decreased with each subsequent pregnancy.
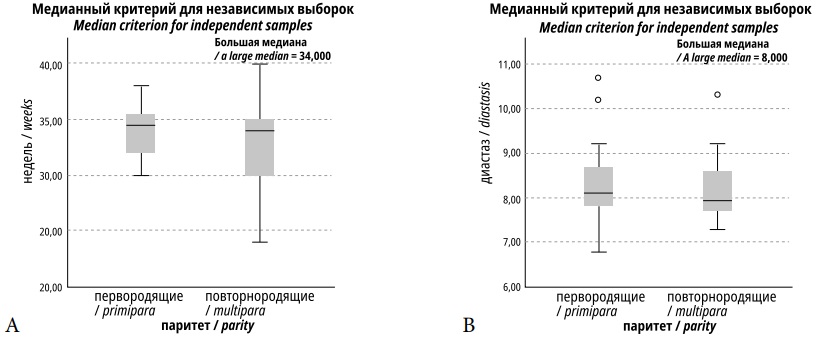
Figure 2. Diagrams showing the distribution of indicators of the time of diagnosis (A), the width of diastasis (B) among pregnant women of 1st group (primipara) and 2nd group (multipara).
The analysis of the anamnesis showed that symphysiopathy was more frequently noted in patients with elevated body weight before pregnancy. BMI 19–24.9 (normal body weight) was in 8 patients (30.7%), BMI 25–30 (increased body weight) in 14 (53.8%), BMI 30.1–34.9 (grade 1 obesity) in 1 (3.8%), BMI 35–40 (grade 2 obesity) in 2 (7.7%), and BMI over 40 (grade 3 obesity) in 1 (3.8%).
The patients were divided into two groups to estimate the significance of BMI in the manifestation of symphysiopathy: Group I – normal BMI, Group II – elevated BMI (including increased body weight and grade I–III obesity).

Figure 3. A diagram showing the structure of the distribution of women into groups with normal BMI and increased BMI.
Table 1
Diastasis of the pubic joint and the time of diagnosis in pregnant women of 1st group (normal BMI) and 2nd group (increased BMI)
|
|
1st group |
2nd group |
Validity of the difference (р) |
|
Diastasis, mm |
7,8±0,59 (6,8-8,8) |
8,8±1,1 (7,0-10,7) |
0,741** |
|
Gestation period, weeks* |
33,6±3,9 (25-38) |
33,1±3,8 (24-40) |
0,612** |
Table 1 shows that pubic articulation diastasis and the time of diagnosis have no statistically significant differences between the normal BMI group and the elevated BMI group, which allows us to exclude BMI as a criterion influencing these parameters.
Pregnancy weight gain averaged 12±4.7 (5–22) kg, which was also normal.
According to the recommended total weight gain depending on a pregnant woman’s BMI [9], patients were divided into two groups. Group I included patients with normal total weight gain, Group II – increased weight gain during pregnancy. A statistical analysis of the possible effect of weight gain on diastasis width was performed; according to the results, the compared groups had a statistical difference in diastasis width (p=0.007). The results are shown in the diagram (Figure 4).

Figure 4. Diagram showing the distribution of diastasis width indicators among pregnant women of 1st group (normal total weight gain) and 2nd group (increased total weight gain).
The analysis of extragenital pathology in the patients of the study group revealed the following diseases: chronic hemorrhoids (n=7 (26.9%)), varicose veins of the lower extremities (n=9 (34.6%)), chronic cystitis (n=2 (7.7%)), chronic pyelonephritis (n=7 (26.9%)), urolithiasis (n=2 (7.7%)), myopia (n=5 (19.2%)), and gestational anemia (n=1 (3.8%)).
The weight of newborns averaged 3436.5±432.9 (2430–4370) g, which was within the normal range.
According to the current scientific literature, sympathetic diastasis of the symphysis over 10 mm wide is considered to be a pubic joint divergence [4][6-11]. However, the assessment of diastasis alone was insufficient, since no reliable relationship was revealed between the severity of diastasis of the pubic bones, on the one hand, and the complaints and clinical symptoms, on the other hand. Logutova et al. (2016) conducted a search for the most significant ultrasound signs of symphysiopathy in pregnant women. The authors found that a discriminant model including the dual contour of the pubic bone, shape change and hypoechogenicity of the superior ligament, and hypoechogenicity of the anterior ligament correctly classified normal and symphysiopathy in 95% of cases. Analysis of the authors’ study data revealed that only three patients (11.5%) had pubic articular diastasis greater than 10 mm, while the remaining 23 (88.5%) patients had diastasis less than 10 mm, but had ultrasound signs of cartilage swelling, which according to modern concepts entitles the diagnosis of "symphysiopathy". [12]. Clinical manifestations of the disease were limited to the assessment of soreness in the pubic region. The pathognomonic sign of symphysiopathy (the occurrence of pain on compression of the greater trochanters and inability to actively bend the hip joints in the prone position assessed) was not assessed in any of the cases [13].
The analysis showed that in the structure of extragenital morbidity, one of the leading places was occupied by diseases of the urinary system (42.3%), which corresponds to the data of Mozgova et al. (2010), who presented a new perspective on the causes of symphysiopathy in pregnant women. According to them, the vast majority (over 80%) of pregnant women with symphysiopathy have urinary tract infections, both chronic and primarily detected during pregnancy. Urinary tract infections are associated with a decrease in calcium and magnesium reabsorption in the renal tubular system, which manifests itself by their increased excretion with urine and leads to a disturbance of mineral exchange [5-7]. As a result, the developing hypomagnesemia (and often magnesium deficiency) leads to a violation of the normal structure of connective tissue, This fact is also confirmed by the present investigation, as the total amount of varicose veins of the lower limbs and chronic hemorrhoids was 61.5%.
The issue of a woman's age as a risk factor for developing symphysiopathy remains controversial. Thus, there are contradictory results of studies devoted to clinical and anamnestic features of women diagnosed with symphysiopathy in the work of Emelyanova (2015), wherein she singles out young age as a risk factor, and the data of Sergeeva (2003), wherein the age group over 26 years old was more prone to develop symphysiopathy than the 16-25-year-old group [1][4][10]. According to the authors’ analysis, the age group older than 26 years old was more than 3 times the age group 19–25 years old. However, there was no statistically significant difference between the two compared groups in terms of the time of diagnosis and width of diastasis as the selected criteria for assessing the course of symphysiopathy.
Currently, there is no unified approach to the treatment and management of patients with symphysiopathy, which is dictated by the restriction of drug intake during pregnancy; therefore, only physical therapy and behavioral therapy, such as wearing a bandage and performing special exercises, are possible, which coincides with the results of the present analysis [8][14][15].
The choice of delivery in symphysiopathy remains unresolved to date. One recent study presented in Logutova et al. (2016) reports that when the total area of structural changes of the interlobar fibrocartilaginous disc (based on the echo-picture of the pubic joint) is up to 50%, delivery through natural childbirth does not increase the risk of pubic joint injury in labor. When the area of changes ranges from 50 to 80%, the prognosis is based on the degree of changes in the pubic symphysis; when the structure changes by more than 80%, the risk of pubic symphysis rupture in vaginal delivery increases [16]. However, at present, the rate of operative delivery of women with symphysiopathy in medical institutions is 100%, which is confirmed by the authors’ data. Probably, the basis of symphysiopathy lies in the gender differences in the symphysis structure and its histological features, which in further studies will help to choose pathogenetic therapy [17].
The present study indicates the lack of significance of such clinical and anamnestic factors as age, parity, and BMI for the manifestation of symphysiopathy in pregnancy. In this study, the only statistically significant criterion affecting the course of symphysiopathy was increased total weight gain during pregnancy.
To date, symphysiopathy remains a pathology with many variables requiring search and clarification, from precise definition and criteria for diagnosis to treatment methods and indications for the choice of a delivery method. A retrospective analysis of the clinical and anamnestic characteristics of women diagnosed with symphysiopathy is one of the steps toward the study of general patterns of this pathology.
1. Dedul' A.G. Increased excretion of calcium and magnesium as a cause of impaired mineral metabolism in pregnant women with symphysiopathy. Journal of obstetrics and women's diseases. 2009; 5: 100. (in Russ.)
2. Normal pregnancy. Clinical recommendations of the Ministry of health of the Russian Federation. - Moscow: publishing house of standards; 2020. 12 р.
3. Emel'yanova D. I. Clinical and anamnestic features of women diagnosed with symphysiopathy during pregnancy in the third trimester from the position of determining bone density.Vyatka medical Bulletin. 2015; 4: 12-15 (in Russ.)
4. Sergeeva O.P. The state of the pubic joint during pregnancy and in the postpartum period according to echography. Kazan medical journal. 2003; 84(4): 261-263 (in Russ.)
5. Mozgovaya E.V. Urinary tract infections in pregnant women. Gestational simpozioane: guidelines: Sankt-Peterburg: N-L; 2008. р.40(in Russ.)
6. Mozgovaya E.V. Dedul' A.G., Oparina T.I., Tkachenko N.N. A new look at the causes of symphysiopathy in pregnant women and the search for effective treatment methods. Journal of obstetrics and women's diseases. 2010; 1: 71-83 (in Russ.)
7. Mozgovaya E. V. Dedul' A.G., Oparina T.I. Evaluation of the effectiveness and safety of calcium therapy in pregnant women with symphysiopathy. Journal of obstetrics and women's diseases. 2013; 62: 10-16. (in Russ.)
8. Çıçek H., Keskın H., Tuhanıoğlu Ü. Simultaneous disruption of the pubic symphysis and sacroiliac joint during vaginal birth. Case Rep Orthop. 2015; 5: 1-5. dOI: 10.1155/2015/812132
9. Hierholzer C., Ali A. Toro arbelaez J.B. Traumatic disruption of pubis symphysis with accompanying posterior pelvic injury after natural childbirth. Am J Orthop (Belle Mead NJ). 2007; 36: 167-170.
10. Laadioui M.,Slimani W., Alaoui F. Disjonction symphysaire apre un accouchement par voie basse dystocique: a propos d’un cas. Pan African Med J. 2014; 17: 33. dOI: 10.11604/pamj.2014.17.33.3441.
11. Shnaekel K.l., Magnan E.F.,Ahma di S. Pubic symphysis rupture and separation during pregnancy. Obstet Gynecol Surv. 2015; 70(11): 713-718. dOI: 10.1097/OGX.0000000000000247
12. Logutova L.S., M.A. CHechneva, N.YU. CHerkasova. Possibilities of predicting the risk of delivery through the natural birth canal in women with symphysiopathy. Russ. Bulletin of obstetrician-gynecologist. 2016; 3: 32-37 (in Russ.)
13. Erickson D., Low J., Shumway J. Management of postpartum diastasis of the pubic symphysis. Orthopedics. 2016;39(2):367-369. DOI: 10.3928/01477447-20160307-02.
14. Urraca-Gesto M.A., Plaza-Manzano G., Ferragut-Garcias A., Pecos-Martin D., Gallego-Izquierdo T., Romero Franco N. Diastasis of symphesis pubis and labor: Systematic review. J Rehabilit Research Develop. 2015;52(6):629-640. DOI: 10.1682/JRRD.2014.12.0302.
15. Mulchandani N.B., Jauregui J.J., Abraham R., Seger E., Illical E. Post-partum management of severe pubic diastasis. Clin Exp Obstet Gynecol. 2017;44(3):464-466. DOI: 10.12891/ceog3533.2017.
16. Logutova L.S. M.A. CHechneva, N.YU CHerkasova. Significant ultrasound signs of symphysiopathy in pregnant women. Theses of the VII Congress of the Association of specialists in ultrasound diagnostics in medicine. 2007; 1:101 (in Russ.)
17. Vorobyеv A.A., Solovyеv O.L., Solovyеv A.O., Pylaeva I.O., Litvina E.V., Bagri E.G.Clinical anatomy of the female perineum. Saint Petersburg; 2021
Alexander A. Vorobyеv, Dr. Sci. (Med.), Professor, Head of the Department of Operative Surgery and Topographic Anatomy
Volgograd
Marina S. Selikhova, Dr. Sci. (Med.), Professor
Volgograd
Marina S. Yakovenko, a postgraduate student of the Department of Obstetrics and Gynecology
Volgograd
Vorobyev A.А., Selikhova M.S., Yаkovenko M.S. Symphysiopathy during pregnancy, assessment of risk factors. Medical Herald of the South of Russia. 2022;13(2):44-49. (In Russ.) https://doi.org/10.21886/2219-8075-2022-13-2-44-49
29, Nakhichevansky Lane, Rostov-on-Don, 344002
Rostov State Medical University
Тel.: +79185710558
e-mail: journal@medicalherald.ru


































